Every pill you swallow, every injection you get, every inhaler you use - it’s not magic. It’s chemistry. Medicines work because they’re designed to interact with your body at a molecular level. But knowing how they work isn’t just for doctors. Understanding how medicines work is one of the most powerful tools you have to use them safely and avoid serious harm.
How Medicines Actually Work
Medicines don’t just float around your body hoping to help. They’re built like keys - each one shaped to fit a specific lock in your cells. These locks are called receptors, enzymes, or transporters. When the right medicine finds its match, it either turns the lock on (an agonist), turns it off (an antagonist), or blocks the keyhole entirely. Take aspirin. It doesn’t just make pain go away. It permanently disables an enzyme called COX-1, which your body uses to make chemicals that cause pain and swelling. No enzyme, no pain signals. Simple. But it’s not always that clean. Some drugs, like lithium for bipolar disorder, don’t have one clear target. They nudge dozens of different systems at once. That’s why lithium needs constant blood tests - too little doesn’t help, too much can poison you. Antibiotics like penicillin work differently. They don’t touch your cells. They attack bacteria by breaking open their walls. Your body’s cells don’t have those walls, so the drug leaves you alone - mostly. That’s why antibiotics don’t work on colds. Viruses don’t have walls to break. Then there are drugs like fluoxetine (Prozac). It doesn’t make you happy. It stops your brain from reabsorbing serotonin, the chemical linked to mood. Think of it like putting a cork in a drain. Serotonin builds up in the space between nerve cells, helping signals flow better. That’s why it takes weeks to work - your brain needs time to adjust.How Your Body Handles Medicine
It’s not enough for a drug to work. Your body has to let it in, move it where it needs to go, and then get rid of it. This is called pharmacokinetics - what your body does to the drug. If you swallow a pill, it travels through your stomach and intestines. But not all of it makes it into your blood. Some gets broken down by your liver before it even gets there. This is the first-pass effect. For drugs like propranolol, up to 90% disappears before it can do its job. That’s why some pills are stronger than others - they’re made to survive your liver. Once in the blood, most drugs cling to proteins. Up to 98% of some medicines, like warfarin, bind tightly to albumin. Only the tiny free portion can act on your body. That’s why mixing warfarin with other drugs - like certain antibiotics - can be dangerous. If the new drug kicks warfarin off the protein, suddenly you’ve got twice as much active drug in your system. That’s when bleeding risks spike. Some medicines need special help to reach their targets. Parkinson’s patients take levodopa because dopamine can’t cross the blood-brain barrier. But levodopa can. It’s like smuggling a key through a locked gate. Once inside, your brain turns it into dopamine.When Medicines Are Safe - And When They’re Not
Safety isn’t about the drug itself. It’s about context. A drug that saves lives in one person can kill another. Warfarin is a perfect example. It’s been used for decades to prevent strokes. But it’s also one of the most dangerous drugs if not managed. Why? Because vitamin K, found in spinach, kale, and broccoli, directly fights its effect. One day you eat a big salad - your INR drops. Next day you skip it - your INR spikes. That’s why people on warfarin are told to eat consistent amounts of greens. Not to avoid them. To keep it steady. MAO inhibitors for depression are another case. They block an enzyme that breaks down tyramine, a chemical in aged cheese, cured meats, and tap beer. If you eat those foods while on the drug, tyramine builds up and causes a sudden, dangerous spike in blood pressure. A single slice of blue cheese can trigger a hypertensive crisis. Patients who know this avoid the risk. Those who don’t end up in the ER. Statins, used to lower cholesterol, are generally safe. But they can cause muscle damage. Why? Because they block HMG-CoA reductase - the same enzyme your muscles need to repair themselves. Most people feel nothing. But if you’re also taking a certain antibiotic or grapefruit juice, your body can’t clear the statin fast enough. Muscle pain becomes a warning sign. Patients who understand this report it early. Those who don’t wait until their muscles start breaking down - a condition called rhabdomyolysis that can lead to kidney failure.
Why Knowing the Mechanism Keeps You Safe
A 2023 study on PatientsLikeMe found that 68% of users worried about side effects. But those who understood how their drug worked? They were 42% less likely to panic over normal symptoms - and 3 times more likely to spot real danger early. Take trastuzumab (Herceptin) for breast cancer. It only works if your tumor has too much HER2 protein. Before treatment, you get tested. If you’re HER2-negative? The drug won’t help. And you won’t waste months on side effects like heart problems - a known risk because HER2 also helps heart cells function. Patients who understood this didn’t just follow the plan. They asked better questions. Even over-the-counter drugs carry risks. Many people think acetaminophen is harmless. But it’s processed by your liver. Take too much, or take it with alcohol, and you can cause liver failure without even knowing it. The maximum daily dose? 3,000 mg - not 4,000 like some labels say. And that includes what’s in cold medicines, pain relievers, and sleep aids you’re taking at the same time.What You Can Do Right Now
You don’t need a medical degree to use medicine safely. Here’s what actually works:- Ask your pharmacist: “What does this drug do in my body?” Don’t settle for “It treats your condition.” Ask how.
- Know your drug’s biggest risk. For statins? Muscle pain. For warfarin? Bleeding. For SSRIs? Withdrawal if stopped cold turkey.
- Check all your meds - including supplements - for interactions. Grapefruit juice affects over 85 drugs. Don’t assume it’s safe.
- Use one pharmacy. They track everything you take and can catch dangerous combinations before you start them.
- Keep a list: drug name, dose, reason, and one key safety tip. Bring it to every appointment.
What’s Changing in Medicine Safety
The FDA now requires drug makers to fully explain how their medicines work before approval. In 2015, only 62% of new drugs had clear mechanism data. By 2023, it was 87%. That’s because drugs with unknown mechanisms cause more harm. They’re harder to dose. Side effects show up late. Trials fail. New tools are coming. The NIH’s All of Us program is collecting genetic data from a million people to see why some people react badly to drugs. Turns out, 28% of bad reactions are tied to genes that change how your body processes medicine. Soon, doctors may use digital twins - computer models of your body - to test how a drug will affect you before you even take it. But that’s years away. Right now, the best tool you have is knowledge.Final Thought
Medicines are powerful. They heal. They save. But they can also hurt - often in ways that seem random, but aren’t. The difference between safety and danger isn’t luck. It’s understanding. When you know how a drug works, you’re not just taking a pill. You’re making an informed choice.Can I stop taking my medicine if I feel better?
It depends on the drug. Antibiotics must be taken fully to kill all bacteria - stopping early causes resistant strains. Antidepressants like SSRIs need time to adjust your brain chemistry - quitting suddenly can cause dizziness, nausea, or anxiety. Blood pressure and heart medications often need to be tapered slowly. Never stop without talking to your doctor - even if you feel fine.
Why do some drugs need blood tests?
Drugs with narrow safety margins need monitoring. Lithium, warfarin, and some seizure meds work in a very small range. Too little = ineffective. Too much = toxic. Blood tests measure how much is in your system so your doctor can adjust the dose. It’s not about checking if it’s working - it’s about making sure it’s not killing you.
Are natural supplements safer than prescription drugs?
No. Supplements aren’t tested like prescription drugs. St. John’s wort can make birth control fail. Kava can damage your liver. Green tea extract in high doses has caused liver failure. Just because something is “natural” doesn’t mean it’s safe. Many supplements interact with prescription drugs in dangerous ways. Always tell your doctor what you’re taking.
Why do some people get side effects and others don’t?
Genetics, age, liver and kidney function, and other medications all play a role. Some people have gene variants that make them process drugs too fast or too slow. Others have weaker livers or kidneys. A drug that’s safe for one person might overload another’s system. That’s why personalized medicine is growing - we’re learning to match drugs to individual biology.
Can I drink alcohol with my medication?
Sometimes, but it’s risky. Alcohol can increase drowsiness with painkillers or anxiety meds. It can raise bleeding risk with warfarin. It can overload your liver when combined with acetaminophen or statins. Even a single drink can be dangerous with certain drugs. If your prescription label doesn’t say “avoid alcohol,” ask your pharmacist. Don’t assume it’s okay.
What should I do if I think I’m having a bad reaction?
Don’t wait. Call your doctor or pharmacist immediately. If it’s severe - trouble breathing, chest pain, swelling, confusion, or severe rash - go to the ER. Report it to the FDA’s MedWatch program. Your report helps others. Keep the medication bottle and note when you took it, what you felt, and when symptoms started. This helps professionals figure out if it’s the drug or something else.
 How Effective Is Calcipotriene for Treating Nail Psoriasis?
How Effective Is Calcipotriene for Treating Nail Psoriasis?
 Quality and Efficacy: Are Authorized Generics as Good as Brand-Name Drugs?
Quality and Efficacy: Are Authorized Generics as Good as Brand-Name Drugs?
 Beclomethasone for Occupational Asthma: Dosing, Safety, and Work-Focused Use
Beclomethasone for Occupational Asthma: Dosing, Safety, and Work-Focused Use
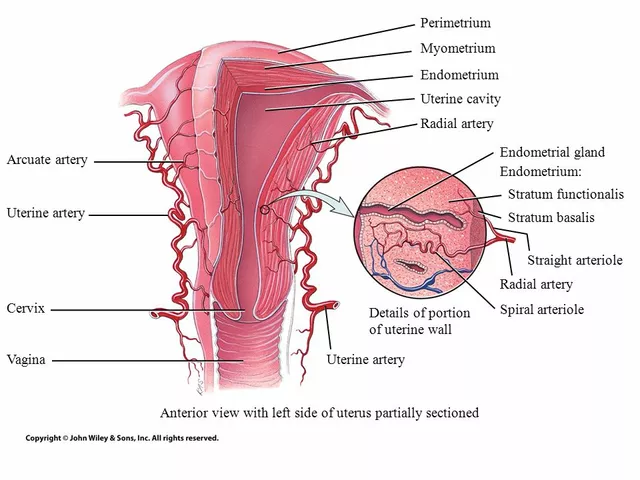 The Connection Between Overgrowth in the Uterine Lining and Migraines
The Connection Between Overgrowth in the Uterine Lining and Migraines
Kristen Yates
December 2, 2025 AT 15:42I used to think pills were just little miracles until my grandma started on warfarin. Now I know why her salad portions are measured like a chemistry experiment. Knowledge really is the only real safety net.
Victoria Graci
December 4, 2025 AT 09:18It’s fascinating how drugs are like silent conductors in an orchestra of biology. Aspirin doesn’t silence pain-it disarms the alarm system. Prozac doesn’t inject joy-it slows the drain on serotonin. We’re not curing symptoms; we’re rewiring the body’s own language. And yet, we still treat medicine like a black box. Maybe the real revolution isn’t new drugs-it’s teaching people to read the manual.
Saravanan Sathyanandha
December 4, 2025 AT 12:25This is one of the clearest explanations of pharmacology I’ve ever read. As someone from India where over-the-counter antibiotics are sold like candy, I’ve seen too many people stop their course because they ‘feel better.’ The consequences are devastating-antibiotic resistance isn’t a buzzword here, it’s a public health crisis. The point about consistent vitamin K intake with warfarin? Crucial. In many cultures, greens are eaten daily, but no one tells them why balance matters. This should be required reading in every community clinic.
Fern Marder
December 5, 2025 AT 21:27GRAPES = 💥 for meds. I didn’t know grapefruit juice could turn my statin into a landmine. Now I check every label like it’s a bomb squad checklist. 🤯 Also, why does no one warn you that your ‘natural’ turmeric supplement is basically a stealth blood thinner? 😭
Carolyn Woodard
December 7, 2025 AT 00:10The pharmacokinetic principles outlined here align with the foundational tenets of clinical pharmacology, particularly regarding first-pass metabolism and protein binding dynamics. The displacement phenomenon observed with warfarin and concomitant medications exemplifies the nonlinearity inherent in drug disposition, which is often underappreciated in primary care settings. Furthermore, the genetic variability in CYP450 enzyme expression-particularly CYP2C9 and CYP2C19-introduces significant interindividual heterogeneity in therapeutic response, reinforcing the necessity for pharmacogenomic screening in high-risk polypharmacy populations.
Anthony Breakspear
December 7, 2025 AT 20:34Man, I used to think my doctor just handed me pills like candy. But after reading this, I started asking my pharmacist how each drug actually works in my body-and wow. I didn’t know my anxiety med was basically a serotonin cork. Or that my statin could wreck my muscles if I drank grapefruit juice. I even made a little cheat sheet for myself: drug, purpose, red flag. Now I bring it to every appointment. Feels like I finally got a seat at the table instead of just being told what to swallow.
Saket Modi
December 9, 2025 AT 16:53why do i need to know all this? just tell me if i can drink beer with my pills or not 😴
Chris Wallace
December 11, 2025 AT 02:07I’ve been on antidepressants for years and never realized they took weeks to work because the brain needs to adapt-not because the drug wasn’t working. I stopped taking mine for a week once because I felt fine, and then the dizziness and nausea hit me like a truck. I thought I was going crazy. Turns out, my brain had rewired itself around the serotonin boost, and pulling the plug was like yanking a power cord out of a running server. Now I taper slowly, and I wish someone had explained this to me in plain language years ago. It’s not weakness to need help-it’s biology. And biology deserves respect.
william tao
December 11, 2025 AT 03:07It is regrettable that the dissemination of such critical pharmacological knowledge remains relegated to the domain of patient advocacy rather than institutionalized medical education. The fact that individuals must independently seek out and comprehend complex biochemical mechanisms to avoid iatrogenic harm constitutes a systemic failure in public health communication. One cannot reasonably expect laypersons to assume the cognitive burden of pharmaceutical risk assessment when regulatory bodies fail to mandate standardized, comprehensible patient-facing pharmacodynamics education. This post, while commendable, is an indictment of a broken system.