
Imagine trying to keep track of ten different pills, each with a different color, shape, and a specific time of day they must be taken. For many seniors, this isn't a hypothetical scenario-it's their daily reality. When a medication list grows too long, the risk of missing a dose or taking the wrong one skyrockets. This is where senior medications is no longer just about the drugs themselves, but about the logistics of taking them. The goal is to move from a chaotic schedule to a streamlined routine that supports independent living without sacrificing health outcomes.
Quick Takeaways for Caregivers and Patients
- Consolidate Timing: Reducing how many times a day a person needs to take pills is the fastest way to improve adherence.
- Combo Products: Switching to fixed-dose combinations can significantly lower the total number of pills.
- Prioritize Deprescribing: Before simplifying, check if every medication is still necessary.
- Professional Help: A clinical pharmacist is the best resource for creating a "best possible medication history."
What exactly is medication regimen simplification?
At its core, medication regimen simplification is a clinical strategy used to reduce the "burden" of treatment. It isn't about changing the medicine's goal-you're still treating the high blood pressure or diabetes-but it's about changing how those medicines are delivered. This might mean moving from a short-acting drug taken four times a day to a long-acting version taken once every morning.
This approach became a formalized part of geriatric care in the 2010s. Experts realized that as the number of seniors taking five or more medications tripled between 1988 and 2010, the old way of prescribing wasn't working. The complexity was causing people to give up or make dangerous errors. By focusing on the process of administration, healthcare providers can help older adults stay in their own homes longer and feel more in control of their health.
The three main ways to reduce pill burden
When looking at a complex list of prescriptions, professionals generally use three primary levers to make things easier. Depending on the health condition, one method may work better than others.
First, there are fixed-dose combination products. These are "all-in-one" pills where two or more active ingredients are combined into a single tablet. For example, instead of taking one pill for hypertension and another for a diuretic, a patient takes one combined pill. This directly reduces the physical number of tablets the person has to swallow.
Second is the shift toward once-daily dosing. Many older medications required dosing every six hours, which is exhausting for a senior and their caregiver. Switching to long-acting formulations means the patient only has to remember their meds once a day, typically during breakfast or before bed.
Finally, the most effective route is often a combined approach-using both combination pills and once-daily schedules. Research indicates that this dual strategy is particularly powerful for complex treatments like antiretroviral therapy, though it may have a smaller impact on common blood pressure or diabetes meds.
| Strategy | Primary Action | Main Benefit | Best Use Case |
|---|---|---|---|
| Fixed-Dose Combination | Combines multiple drugs into one pill | Fewer total pills to swallow | Hypertension, Cholesterol |
| Once-Daily Dosing | Uses long-acting formulations | Fewer administration times per day | Chronic pain, Mental Health |
| Combined Approach | Reduces both pill count and frequency | Maximum reduction in treatment burden | Complex HIV or autoimmune regimens |

The step-by-step path to a simpler routine
You can't just start moving pill times around without a plan. There is a structured pathway that healthcare providers follow to ensure safety. If you are managing care for a loved one, this is the process you should advocate for with their doctor.
- Create a "Best Possible Medication History": This is a deep dive. A pharmacist spends 30 to 60 minutes reviewing every single bottle in the house, including over-the-counter supplements and old prescriptions that might still be in use. It's common to find a gap between what the doctor thinks the patient is taking and what is actually happening at home.
- Assessment of Appropriateness: Before simplifying, the provider asks: "Does this person actually still need this drug?" This is known as deprescribing. Removing an unnecessary medication is the ultimate form of simplification.
- Identify Simplification Opportunities: Using tools like the MRS GRACE guide, the pharmacist looks for ways to consolidate times. For example, if a patient takes meds at 8 AM, 12 PM, 4 PM, and 8 PM, can some of those be moved to just 8 AM and 8 PM?
- Patient and Caregiver Consultation: This is a critical step. A regimen that looks perfect on paper might fail if it conflicts with the patient's life. If a patient hates taking pills in the morning, moving everything to the evening is a win, even if it's not the "standard" clinical time.
- Implementation and Follow-up: The new plan is put into action, and the patient is monitored to ensure the changes haven't negatively impacted their clinical outcomes.
Common roadblocks and how to handle them
Simplification isn't always a straight line. There are "hard rules" in pharmacology that can't be ignored. For instance, thyroxine (used for thyroid issues) usually needs to be taken on an empty stomach before breakfast to be absorbed. Trying to move it to a dinner-time block just for simplicity would make the drug less effective.
Similarly, some statins for cholesterol are better taken at night. When these "pharmacokinetic" requirements clash with the goal of simplification, the clinical need wins. The trick is to simplify everything else around these non-negotiable medications. The goal isn't 100% perfection, but a significant reduction in total effort.
Another challenge is the time it takes. Comprehensive reviews can take nearly an hour per patient, which is a lot in a busy clinic. However, the payoff is huge. One facility using a standardized simplification tool reported a 30% drop in medication errors. When the staff isn't rushing to manage twenty different schedules, they make fewer mistakes.
Why this matters for the future of care
We are facing a global demographic shift. The UN predicts that the number of people aged 65+ will double by 2050. If we continue to add pills to regimens without simplifying them, we will see a crisis of non-adherence. We've already seen the trend in the US, where polypharmacy-the use of many medications-has become the norm rather than the exception.
New technology is starting to help. Some electronic health records now include complexity scoring tools that alert doctors when a patient's regimen has become too difficult to manage. Germany has even introduced reimbursement incentives for pharmacists who perform these simplification reviews. It's a shift in thinking: we aren't just treating a disease; we're treating a person who has to live with the treatment every single day.
Does simplifying medications make them less effective?
Not if done correctly. Simplification focuses on the delivery method (timing and formulation) rather than the therapeutic intent. By using long-acting versions or combination pills, the actual dose of the medication remains the same. In many cases, simplification actually increases effectiveness because the patient is much more likely to take their medication consistently and correctly.
What is the "best possible medication history"?
It is a comprehensive list of all medications a patient is actually taking, created by comparing pharmacy records, physician notes, and a physical inspection of the medications in the patient's home. It is the gold standard for preventing errors because it catches discrepancies, such as a patient taking a generic version of a drug that the doctor has listed as a brand name, or using a supplement that interacts with a prescription.
Can I simplify my parents' medications without a doctor?
No. You should never change the timing or formulation of a prescription without professional guidance. Some medications have very specific absorption requirements or interact with others if taken at the same time. Always start by requesting a "medication regimen review" from their primary care physician or a clinical pharmacist.
What is the difference between simplification and deprescribing?
Deprescribing is the process of identifying and stopping medications that are no longer needed or are causing more harm than good. Simplification is the process of making the remaining necessary medications easier to take. Ideally, a provider will deprescribe first to remove any unnecessary pills, then simplify the rest of the regimen.
How often should a medication regimen be reviewed for simplification?
Generally, a full review should happen at least once a year, or whenever there is a major change in health, such as a new diagnosis, a hospital discharge, or a change in the patient's ability to self-manage their meds. Because health needs change as we age, a regimen that worked two years ago might be too complex today.
Next Steps for Better Management
If you're feeling overwhelmed by a complex pill schedule, don't try to fix it alone. Start by gathering every single bottle, cream, and supplement into one bag. Schedule a dedicated appointment with a pharmacist or doctor specifically for a "medication review," rather than trying to squeeze it into a standard 15-minute check-up. Be honest about which pills are the hardest to remember and where the routine is breaking down. The goal is a plan that fits your life, not a plan that forces you to live around your medicine.
 Feldene (Piroxicam) vs Topical NSAID Alternatives - Pros, Cons & Best Uses
Feldene (Piroxicam) vs Topical NSAID Alternatives - Pros, Cons & Best Uses
 Buy Generic Premarin Online? Safe Options, Cheaper Estradiol Alternatives, and 2025 Prices
Buy Generic Premarin Online? Safe Options, Cheaper Estradiol Alternatives, and 2025 Prices
 How to Keep a Medication List for Safer Care and Fewer Errors
How to Keep a Medication List for Safer Care and Fewer Errors
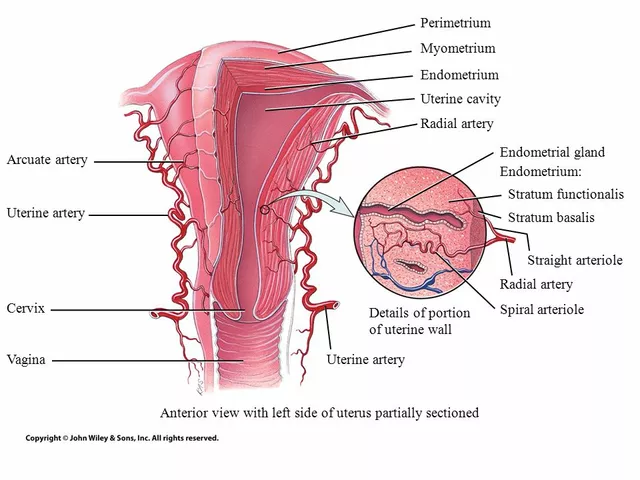 The Connection Between Overgrowth in the Uterine Lining and Migraines
The Connection Between Overgrowth in the Uterine Lining and Migraines