One in five children in the U.S. has obesity. That’s not a distant statistic-it’s your neighbor’s kid, your child’s classmate, maybe even your own child. And while it’s easy to blame junk food or too much screen time, the real issue runs deeper. Childhood obesity isn’t just about what kids eat. It’s about what the whole family does, day after day. The good news? There’s a proven way to turn this around, and it doesn’t involve strict diets or shame. It’s called family-based treatment, and it’s the most effective approach doctors now recommend.
Why Family-Based Treatment Is the Gold Standard
For decades, doctors tried treating childhood obesity by focusing only on the child. Give them a meal plan. Tell them to exercise more. But results were poor. Kids often regained the weight, and families felt overwhelmed. Then came research from Dr. Leonard Epstein and his team at the University at Buffalo in the 1980s. They flipped the script: instead of targeting the child alone, they trained parents to create a healthier home environment. The results? Children lost weight-and kept it off. Parents lost weight, too. Today, the American Academy of Pediatrics, the American Psychological Association, and the National Institutes of Health all agree: family-based behavioral treatment (FBT) is the gold standard for kids aged 2 to 18. Why? Because kids don’t live in a vacuum. They eat what’s in the fridge, watch TV in the living room, and copy what their parents do. If mom drinks soda daily, or dad skips meals, or the whole family eats in front of the TV, changing the child’s behavior alone is like trying to fill a leaky bucket. A major 2023 JAMA Network Open trial followed 306 families over two years. Kids in the FBT group lost 12.3% more of their excess weight than those in usual care. Parents lost 5.7% more weight. Even siblings who weren’t directly part of the program saw a 7.2% improvement in their weight. That’s not a coincidence. When the family changes, the child changes with it.What Family-Based Treatment Actually Looks Like
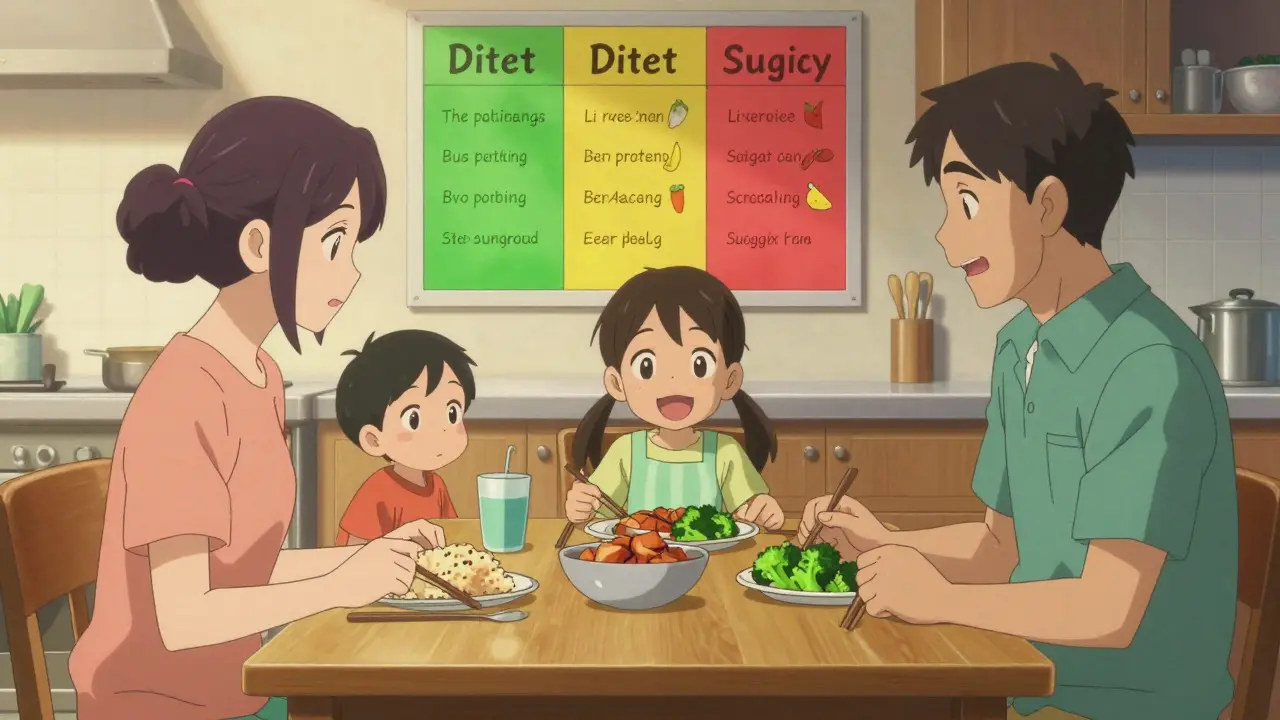
FBT isn’t a quick fix. It’s a structured program, usually 16 to 32 sessions spread over 6 to 24 months. Most are done in a pediatrician’s office, not a specialty clinic. That’s key-92% of kids see a pediatrician regularly, but only 12% ever visit a weight clinic. Bringing treatment into primary care removes barriers like travel, cost, and stigma. The core of FBT? Four pillars:- Nutrition using the Stoplight Diet: Foods are grouped into three colors. Green = eat freely (fruits, veggies, whole grains). Yellow = eat in moderation (dairy, lean meats, nuts). Red = eat sparingly (soda, candy, fried foods). No food is banned. Kids learn to make smarter choices without feeling punished.
- Physical activity: At least 60 minutes a day of moderate to vigorous play-biking, dancing, soccer, even brisk walking. It’s not about sports teams. It’s about moving more, every day.
- Behavior tracking: Families keep simple logs of what they eat and how much they move. Not to judge, but to spot patterns. Did they eat out more on weekends? Did screen time spike after school? Awareness leads to change.
- Parenting skills: This is where most programs make the biggest difference. Parents learn how to set limits without yelling, reward effort instead of weight loss, and avoid using food as comfort or punishment. They learn to say, “Let’s go for a walk,” not, “You’re getting too fat.”
How the Stoplight Diet Works in Real Life
The Stoplight Diet isn’t theoretical. In Epstein’s studies, kids using it lost an average of 9.38% of their excess weight in just six months. Here’s how it plays out in a real home: Instead of keeping chips and cookies on the counter, a family puts them in a high cabinet. They keep apples, carrots, and yogurt at eye level. At dinner, they serve a plate with half veggies, a quarter lean protein, and a quarter whole grains. Soda is replaced with sparkling water or milk. Dessert? A small portion of fruit, not ice cream. The trick? Consistency. A child who eats green foods at school but comes home to red foods every evening won’t make progress. The whole household has to align. That’s why FBT requires at least one parent to be fully involved. When parents model healthy eating, kids follow. One study found that when parents cut out sugar-sweetened drinks, their kids’ BMI dropped by 1.0 unit in just 12 months.Why Siblings and Parents Also Lose Weight
One of the most surprising findings in recent FBT research? You don’t have to treat every child in the family for all of them to benefit. In the 2023 JAMA trial, siblings who weren’t even part of the program lost weight. Why? Because the family’s habits changed. The fridge was stocked differently. Dinners were eaten together. Walks after dinner became routine. The kids who weren’t targeted still ate the same meals, moved more, and watched less TV. Their bodies responded. Parents lost weight, too. That’s not an accident. FBT doesn’t just change the child’s behavior-it changes the family’s. When parents learn to cook healthier meals, they lose weight. When they start walking after dinner, they get more active. When they stop using food to soothe stress, they improve their own mental health. This ripple effect is powerful. It means FBT isn’t just a treatment-it’s a lifestyle upgrade for the whole family.
When Family-Based Treatment Isn’t Enough
FBT works best for most kids. But it’s not a magic bullet. For children with severe obesity-those with a BMI at or above 120% of the 95th percentile-FBT alone often isn’t enough. In these cases, fewer than half of kids lose even 5% of their body weight after a full year of treatment. That’s when doctors consider other options. For teens, medications like semaglutide (Wegovy) or liraglutide (Saxenda) can help. For those with extreme obesity and related health problems, metabolic surgery may be an option. But these aren’t first steps. They’re next steps. FBT still comes first. The American Academy of Pediatrics says: start with FBT. If progress stalls after 6 months, then add other tools. Don’t skip the family part. Even when meds are used, families still need to support healthy eating and activity. Otherwise, the gains won’t last.Barriers to Getting Help-and How to Overcome Them
FBT is proven. But it’s still underused. Only 5% of eligible kids get it. Why?- Doctors don’t offer it. Many pediatricians aren’t trained in behavioral techniques. They don’t know how to start the conversation.
- Families are overwhelmed. Juggling work, school, and appointments is hard. Many parents feel guilty or ashamed and avoid the topic.
- Cost and access. Insurance often covers FBT under the G0447 code for intensive behavioral therapy, but many practices don’t bill it correctly. Low-income families, especially Hispanic and Black families who make up over half of obese children, are less likely to get referred.
What Parents Can Do Today
You don’t need to wait for a referral. You don’t need to wait for a doctor to bring it up. Here’s what you can start tomorrow:- Make one meal a day a family meal. No phones. No TV. Just eating together. Studies show this cuts obesity risk by 12%.
- Swap one sugary drink for water or milk. That one change can drop a child’s BMI by 1.0 unit in a year.
- Limit screen time to under two hours a day. That’s not counting homework. That’s YouTube, TikTok, games. Every extra hour adds 0.8 BMI units.
- Be the example. If you want your kid to eat more veggies, eat them yourself. If you want them to move more, go for a walk after dinner. Kids copy what they see.
- Don’t wait. Experts say if you wait until a child is severely obese, it’s much harder to reverse. Start now-even if the child is only 4 or 5.

What the Future Holds
The future of childhood obesity treatment is hybrid. Apps that track meals and activity. Text reminders for family walks. Video coaching for families who can’t make it to the office. The 2023 AAP guidelines now recommend combining in-person FBT with digital tools. In pilot studies, this boosted engagement by 32%. The government is starting to catch up. Medicare now covers FBT. The Inflation Reduction Act funds community programs. More pediatric practices are hiring behavioral health coaches. But technology alone won’t fix this. What fixes it is connection. A parent who sits down with their child and says, “Let’s try this together.” A family that learns to eat, move, and live differently-not because they have to, but because they want to.Frequently Asked Questions
Is childhood obesity just about eating too much?
No. While diet plays a role, childhood obesity is caused by a mix of factors: genetics, environment, stress, sleep, and family habits. A child who eats healthy food but watches TV all day and sleeps less than 9 hours is still at high risk. It’s not just about calories-it’s about routines, stress levels, and how the family functions together.
Can I do family-based treatment at home without a program?
Yes, you can start using the principles right away. Use the Stoplight Diet to reorganize your fridge. Make meals screen-free. Aim for 60 minutes of daily movement. Track your family’s habits for a week to spot patterns. But for lasting results, especially if your child is significantly overweight, working with a trained coach increases success by 3 to 4 times. Professional support helps you stay consistent and avoid common mistakes.
Will my child be shamed or blamed in family-based treatment?
No. FBT is designed to be supportive, not punitive. Coaches avoid words like “fat,” “obese,” or “diet.” Instead, they focus on behaviors: “What did you eat today?” “How did you feel after dinner?” “What made it hard to be active?” The goal is to build confidence, not guilt. Research shows shame makes weight loss harder, not easier.
How long does family-based treatment take to work?
Most families see small changes in 4 to 6 weeks-like better sleep, more energy, or fewer snacks between meals. Weight loss usually starts after 3 to 4 months. The full program lasts 6 to 24 months, with 26 sessions recommended. The longer families stick with it, the more lasting the results. Kids who complete the full program are 2.3 times more likely to keep the weight off five years later.
Is family-based treatment covered by insurance?
Yes, under Medicare and most private insurers, intensive behavioral therapy for obesity (CPT code G0447) is covered. Each 15-minute session is reimbursed, and up to 26 sessions over 12 months are recommended. But many practices don’t bill for it. Ask your pediatrician if they offer FBT and if they accept G0447. If not, ask them to connect you with a local program that does.
 Affordable Rifaximin Alternatives for IBS-D and Traveler’s Diarrhea Relief
Affordable Rifaximin Alternatives for IBS-D and Traveler’s Diarrhea Relief
 Why Setting Boundaries Is Crucial for Living with Depressive Disorder
Why Setting Boundaries Is Crucial for Living with Depressive Disorder
 Level Up Your Health: Why Silicon Supplements Are Your New Secret Weapon
Level Up Your Health: Why Silicon Supplements Are Your New Secret Weapon
 Female Cialis (Tadalafil) vs. Alternatives: Pros, Cons & Best Choices
Female Cialis (Tadalafil) vs. Alternatives: Pros, Cons & Best Choices
 Serum Sickness-Like Reactions to Antibiotics: What Parents and Doctors Need to Know
Serum Sickness-Like Reactions to Antibiotics: What Parents and Doctors Need to Know
Amy Vickberg
January 16, 2026 AT 10:19My husband and I started using the stoplight diet last month after our daughter was flagged at her checkup. We didn’t even realize how much soda we were drinking until we tracked it. Now we keep sparkling water in the fridge and fruit on the counter. She’s happier, sleeps better, and we’ve all lost a few pounds without even trying. It’s not perfect, but it’s real.
Thank you for writing this. It feels like someone finally gets it.
Haley Graves
January 17, 2026 AT 17:04I work as a pediatric nurse and I’ve seen this work over and over. The families who succeed aren’t the ones with the most willpower-they’re the ones who stop treating food like a weapon and start treating it like a tool. The real magic? When parents stop saying ‘you need to lose weight’ and start saying ‘let’s do this together.’ That shift changes everything.
And yes, it’s hard. But so is watching your kid get bullied at school because of their size. This is the better fight.
Gloria Montero Puertas
January 19, 2026 AT 00:49Let’s be honest: this is just another form of liberal social engineering dressed up as ‘health.’ The real problem? Parents have abdicated their authority. They’ve turned feeding into a democracy, and now children rule the kitchen. No wonder obesity is rampant. The solution isn’t ‘family-based treatment’-it’s discipline. Set boundaries. Say no. Stop coddling. Stop rewarding bad behavior with snacks. Simple. Direct. Effective.
And for the record: ‘stoplight diet’ sounds like something a kindergarten teacher would use to teach traffic rules-not nutrition science.
Frank Geurts
January 20, 2026 AT 10:17As someone who grew up in a household where meals were sacred, communal, and culturally rooted, I find this article profoundly aligned with traditional values. In my Indian-American home, we never ate in front of screens. We ate together. We shared. We sipped buttermilk, not soda. We walked after dinner-not because it was prescribed, but because it was ritual.
The brilliance of family-based treatment is not its novelty-it’s its return to the human rhythm of eating, moving, and connecting. Modern medicine has forgotten this. The data confirms what our grandparents knew: health is a collective act, not an individual burden.
Thank you for honoring that truth.
Arjun Seth
January 20, 2026 AT 21:51This is all nonsense. Obesity is caused by sugar and carbs. That’s it. No family nonsense. No behavioral therapy. Just cut the bread, the soda, the rice. Eat meat and vegetables. Done. The fact that doctors are wasting time on ‘parenting skills’ and ‘stoplight diets’ proves how broken the system is. You don’t need a coach. You need a knife. Cut the carbs. That’s it. Why are we making this so complicated? People used to be thin because they didn’t have access to processed food. Simple. Not rocket science.
Mike Berrange
January 22, 2026 AT 16:49So let me get this straight: you’re telling me that if I just move the cookies to a high cabinet and say ‘let’s go for a walk,’ my 14-year-old will magically lose weight? And you’re not even addressing the underlying trauma? The emotional eating? The anxiety? The fact that 70% of obese kids have at least one parent with depression? You’re treating symptoms, not causes. And you’re calling this ‘gold standard’? That’s not medicine. That’s a feel-good pamphlet.
Also, ‘no food is banned’? So you’re okay with a kid eating 12 donuts a day as long as they’re ‘aware’? That’s not therapy. That’s negligence.
Dan Mack
January 24, 2026 AT 07:37They’re hiding the real agenda. This isn’t about health. It’s about control. The same people pushing ‘family-based treatment’ are the ones pushing school lunches with kale and no pizza. The same ones who want to ban soda in vending machines. The same ones who call your kid ‘obese’ to get funding. This is a stealth way to regulate parenting. You think this is voluntary? Wait until the IRS starts auditing your grocery receipts. Wait until your kid’s school reports you for ‘unhealthy household habits.’
They’re not helping kids. They’re building a surveillance state under the guise of ‘wellness.’
Nishant Garg
January 25, 2026 AT 16:12I come from a small village in India where kids ran barefoot until sunset, ate whatever was cooked-roti, dal, seasonal veggies-and never heard the word ‘obesity.’ We didn’t count calories. We didn’t have stoplights. We had rhythm. We had community. We had grandparents who taught us to eat slowly and share what little we had.
What’s missing in America isn’t a diet plan-it’s presence. Not the kind you track in an app. The kind you feel in a quiet kitchen, with laughter, with no screens, with someone saying, ‘Here, have my portion.’
FBT is brilliant because it’s not new. It’s old wisdom, repackaged. And honestly? It’s beautiful. The science just caught up to what our ancestors knew. Let’s not overcomplicate it. Bring back the table. Bring back the togetherness. The rest follows.
Jan Hess
January 26, 2026 AT 00:07My kid was at 98th percentile. We started with one change: no screens during dinner. That’s it. One week later, he asked for an apple instead of chips. Two months in, he’s running around the yard like he’s chasing fireflies. We didn’t even talk about weight. We just ate together. Walked together. Laughed together.
It’s not about fixing your kid. It’s about fixing your life. And honestly? I’m glad I did it. We’re all better for it.